Introduction
The patient was a 61-year-old, extremely obese, white male who complained of acute abdominal pain. The episode began approximately 2 weeks earlier with a mild attack of abdominal pain and intense nausea unrelieved by a laxative. After resting in bed for about a day, he was able to resume some activities, although he felt weak and was easily fatigued.- Past medical history: typhoid fever at age 30, no other serious illnesses
- Social history: smoked heavily and was a moderate-to-heavy drinker
- Family history: 2 relatives died from gastric cancer
- Physical examination: obese male in obvious distress, positive physical findings limited to the abdomen, where there was marked tenderness, especially on the right side, and a sensation of a mass in the iliac fossa
- System review: negative except for marked obesity
- Course of illness: abdominal pain persisted, becoming much more severe over the next 10 days; loss of appetite, eating only small amounts of light food; continued bouts of fever and abdominal pain; an operation was performed on the 10th day after the onset of symptoms
This famous patient was King Edward VII, son of Queen Victoria. The Queen died in 1901 and Edward, who had waited many years in line for the throne as the Prince of Wales, was to be crowned king on June 26, 1902. But about 2 weeks before this much-heralded event, Edward became ill with appendicitis -- a disease that, at the beginning of the 20th century, was only beginning to be diagnosed and had a high mortality rate.
At first, Edward adamantly refused to consider the possibility of surgery because it would mean postponing his highly anticipated coronation, and because appendectomy was not widely accepted in 1902. The King's physicians suggested that Frederick Treves, a surgeon, be called to examine the seriously ill patient. Treves, who had lectured and written about appendicitis (then called "perityphilitis") recommended an operation, but the King protested: "I have a coronation on hand." Treves replied, "It will be a funeral if you don't have the operation."[1]
Finally, the King consented and the operation, which lasted less than an hour, took place at Buckingham Palace. Treves located and drained an appendiceal abscess without removing the appendix. After the King's swift recovery, the coronation was held on August 9, 1902.
Appendicitis is no longer considered a diagnostic or surgical challenge, but at the beginning of the 20th century, little was known about the disease or its treatment. Although there had been discussion that excision of the obstructed appendix was the best way to treat the disease, delayed surgery to allow time for the formation of a walled-off abscess was believed to be the safest method. This is the course that Treves followed.
Appendicitis remains the most common reason for abdominal surgery in young adults.
Current surgical strategy focuses on early diagnosis and excision of the appendix, even if there is an associated abscess. The case fatality rate for appendicitis is about 2-3 per 1000 attacks with higher rates observed in very young and older patients. As we enter the 21st century, it is unclear why the incidence of appendicitis has decreased over the past several decades, and whether this decline might be due to a change in diet or is reflective of more accurate diagnosis. Several questions about appendicitis are frequently asked.
Is Computerized Tomography (CT) Indicated as a Diagnostic Aid?
CT scans improve diagnostic accuracy, but take time and add to the cost of care. CT scans are best employed when there is diagnostic uncertainty, such as in older patients; in geographic regions where appendicitis is infrequent; or in females, in whom appendicitis can be easily confused with gynecologic conditions. If a person such as Edward VII developed symptoms and signs of appendicitis today, it is likely that a CT scan would be ordered, not so much because of who he is, but because of his age.Figure 1 shows a CT scan from an 18-year-old female who presented with a 2-day history of mid-abdominal pain that was treated with ranitidine (Zantac). She presented to the emergency department 4 days later with sudden onset of diaphoresis, nausea, vomiting, and loose stools. The patient described a classical history of appendicitis with initial mid-epigastric pain, lasting approximately 2 days, which shifted to the right lower quadrant. At surgery, a necrotic appendix was removed. The adjacent peritoneal fluid was infected; therefore the surgical wound was left open, anticipating a delayed primary closure. The patient's clinical course was further complicated by a wound infection, which required intravenous antibiotics.
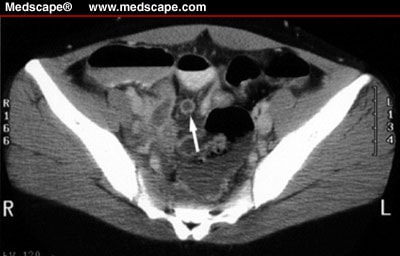
Figure 1. Computerized tomography scan from patient with acute appendicitis. Intravenous contrast-enhanced CT image of the pelvis demonstrates dilated, fluid-filled appendix (arrow). In this case, rectal contrast was not necessary to differentiate the inflamed appendix from surrounding bowel. With permission of Dr. Arun Vade, Loyola University Medical Education Network.
Is Laparoscopic Surgery Superior to the Conventional Right Lower Quadrant Open Surgical Approach?
Appendectomy can usually be performed through a small incision, allowing for a quick recovery after only a brief hospitalization. Hospitalization may be slightly shorter after laparoscopic appendectomy, but laparoscopic surgery is more expensive. If surgical reimbursement rates are low, open appendectomy is cost-effective for patients younger than 35 years of age.When Should a Surgeon Perform "Incidental" Appendectomy?
Based on the frequency of appendicitis, incidental appendectomy is indicated when feasible during performance of abdominal operations in younger patients.As a follow-up to this case, King Edward lived another 8 years without further attacks of appendicitis before dying of heart disease in 1910. Frederick Treves, the intrepid surgeon, was eventually knighted. Ironically, despite Treves' interest in and knowledge about appendicitis, his daughter died from the disease.
References
- Frederick Treves (1853-1923). The Dorset Page. Available at: http://www.thedorsetpage.com/people/Frederick_Treves.htm. Accessed April 2, 2002.
Authors and Disclosures
Albert B. Lowenfels, MD, Professor of Surgery, New York Medical College, Valhalla, New YorkMedscape General Surgery. 2002;4(1) © 2002 Medscape
Thanks for your great information, the contents are quiet interesting.Keep updating more information from your blog.I will be waiting for your next post.
Trả lờiXóaInfertility Surgery Treatment in Bangalore | Gynecologist in Bangalore| Best Pelvic Floor Surgery Doctor in Bangalore | Vaginal Hysterectomy Surgery in Bangalore